How Clinician-Led Innovation Makes a Difference
5 min read
Summary. More and more hospitals are looking to doctors and nurses for insights to create and implement innovative solutions in care delivery (Kuhrt, 2017). This is Clinician-Led Innovation, and it leverages three core elements that are design thinking, feedback loops/effective communication, and interdisciplinary collaboration.
1. Design thinking.
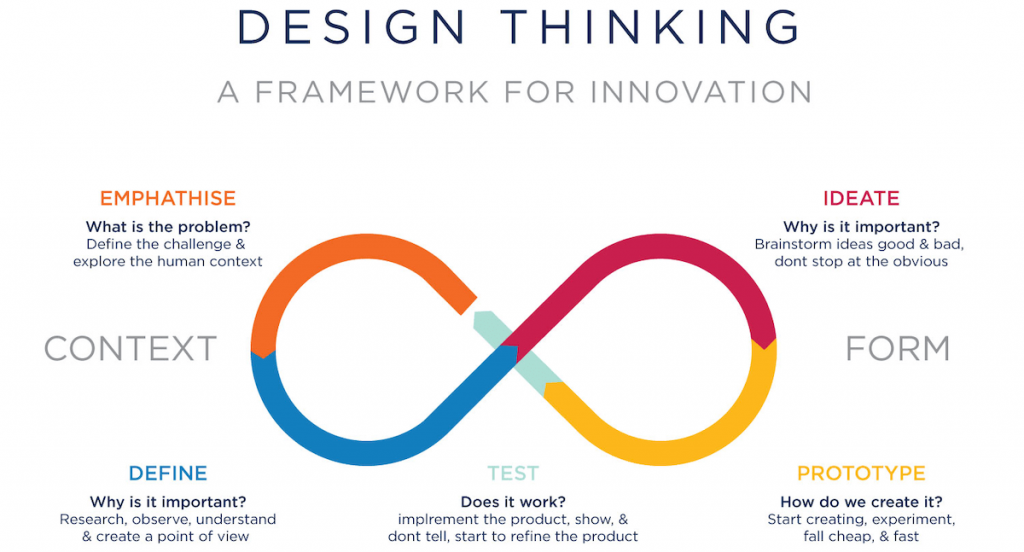
Have you noticed that even when we stimulate new ideas, we often struggle to apply them? This happens because individual biases and entrenched behaviours get in the way and paralyse the opportunity. Design thinking is a set of cognitive, strategic, and practical processes that helps to develop concepts by following a methodology where you define the problem, experiment, test, and learn from the results (Figure 1). It assists teams to overcome biases and to unleash their creativity. Insights from differing experiences are used to reshape problems and solutions (Liedtka, 2018, (OZ, 2020)).
‘Design Thinking for Doctors and Nurses’ in the New York Times shows how simple insights can bring positive outcomes such as orange vests for trauma team leaders to identify them more easily during chaotic procedures or a pain scoring system simplified for easier use in paediatric wards (Kalaichandran, 2017).
2. Feedback loops and effective communication.
Innovation is only as good as the weakest link. The road to healthcare innovation is paved with good communication — from the top-down, the bottom up, and horizontally across the care delivery continuum. For example, Boston Children’s Hospital launched an internal accelerator program to facilitate getting ideas and insights off the paper and into practice (Minemyer, 2017).
Innovation requires consistent effort to weave communication best practices into an organisation’s culture:
- An open-door policy among leadership,
- Regular informal contact to uncover insights,
- Encouraging managers, clinicians and patients to provide feedback, and
- Making actions from feedback visible,
- to provide reinforcement that feedback loops ultimately improve care delivery.
3. Interdisciplinary collaboration.
Interdisciplinary collaboration requires people from different professional fields – not merely different healthcare disciplines. Examples include utilising architectural and engineering inputs to a common goal – improved healthcare outcomes (Gang, 2017):
- Bon Ku, M.D., director of the Jefferson Health Design Lab, University in Philadelphia, matched medical with architecture students to develop a tool that tracks clinical staff and patients as they move around the emergency room (Kalaichandran, 2017)
- The University of Washington’s engineering program has been reaching out to clinicians seeking to collaborate on innovative medical device designs. One project involved developing a cheaper, refillable version of the EpiPen in response to price jumps for the device that occurred last year (Long, 2019, Sweeney, 2016).
4. Clinical engagement and leadership
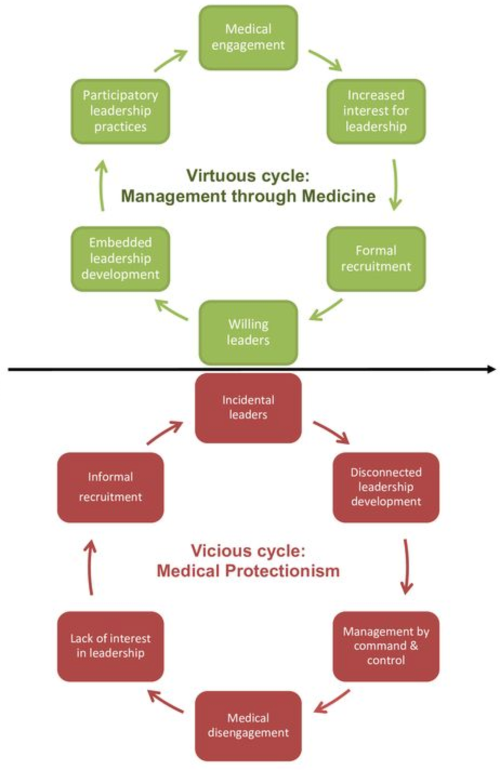
The traditional approach in healthcare divides care from the administration (Figure 2). Doctors and nurses look after patients, owning care processes, while administrators look after the organisations that treat them (Savage, et al., 2020).
Understanding the interdependence of clinical processes and administrative processes and learning leadership skills helps clinicians, and the organisation, achieve their objectives. Engaging clinicians is most effectively achieved by providing tools and systems to unlock their leadership capabilities (Fahlbusch, 2019).
A new leadership style is to transform healthcare by stimulating innovative insights mainly from doctors and other clinicians. Clinicians have the expertise to make frontline decisions to determine the quality and efficiency of care and the technical knowledge to provide better strategic choices about service delivery in the longer term. There are three types of clinical leadership.
- Executive-level clinical leaders have a deep, broad understanding of both care and administration. Therefore, skills such as strategic thinking, planning, communication, negotiation and influence are expected from this leader.
- Service leaders are passionate advocates of their units or teams, who are also aware of the context and requirements of the whole organisation.
- Frontline leaders are clinicians who focus on the direct delivery of patient care and see continuous improvement in the way the organisation delivers care as their responsibility (Mountford, 2009).
These three levels of leadership are equally important. Although executive-level clinical leaders and service leaders have greater overall responsibility, frontline leaders ultimately hold the key to applying the organisation’s vision by using their day-to-day experience to notify the constant improvement of services. Clinicians on different “levels” are likely to be peers with similar remuneration and professional status but varying degrees of leadership focus, engagement, and specialisation (Mountford, 2009).

Professor Christine Jorm, a world authority on medical education and expert on workforce engagement, put together a summary of actions to help Safer Care Victoria develop a cohesive long-term strategy for strengthening clinician engagement in Victoria. (Figure 3).
Many gaps in clinical engagement can be mitigated or eliminated resolved altogether. The solutions are designed to influence clinician engagement at multiple levels and address the complex healthcare delivery system. (Jorm, 2017)
5. Study case – Kaiser Permanente
The company struggled with worsening clinical and financial performance and losing its best clinicians in the late 1990s. Jack Cochran, the new executive medical director and a paediatric plastic surgeon, made clinical leadership a solid force to improve outcomes for patients. He revamped the clinician’s role as “healer, leader, and partner” and the company’s leadership-development programs for doctors. Within five years, Colorado had become Kaiser’s highest-performing affiliate on quality of care and a beacon of quality within US health care. Patients were significantly more satisfied, staff turnover fell dramatically, and net income rose from zero to $87 million.
Conclusions.
Clinicians are unexploited resources with huge potential for innovation. The pressure of daily clinical life impairs clinicians’ ability to stop, take a breath and think; what could be improved here? The main lessons are to create a culture that encourages clinicians to have a business mindset; give and receive constructive criticism; provide quick replies to proposals, and seek leaders with entrepreneurial vision (Minemyer, 2017).
By encouraging design thinking, feedback loops, and interdisciplinary collaboration, clinicians’ unique insights can support and drive excellence in innovation in healthcare, which is crucial to create better care.
Further reading:
- Fahlbusch, D.: Reimagining Healthcare – How clinicians and non-clinicians reduce risk, waste and disjointed services
- Fierce Healthcare: Despite constraints, innovation is necessary in hospital design
- Safer Care Victoria – Clinical engagement Framework – Clinicians as partners
- New York Times: Design Thinking for Doctors and Nurses
- Fierce Healthcare: Clinician-driven innovation on the rise
- Harvard Business Review: Why design thinking works
- Seattle Times: Students create innovative devices to solve vexing medical problems
- Fierce Healthcare: 4 lessons from Boston Children’s innovation program
- McKinsey Quarterly: When clinicians lead
- UX beginner: UX Design Processes
- BMJ Journals: Medical leadership: boon or barrier to organisational performance?



